

What is Refractive Errors?
In normal vision (emmetropia), light rays from an object focus onto the retina. Under normal conditions, as the eyeball grows in size from infancy to adulthood, there will be a corresponding change in curvature of cornea and the lens, enabling the eye to remain emmetropic, at all ages.
Refractive error occurs, in one or more of the following situations:
- The eyeball being larger or smaller than the normal size
- The corneal curvature being flatter or steeper than usual
- Increase or decrease in the power of the lens

What are the symptoms of Refractive Errors?
The child or patient should be checked by an ophthalmologist, if any one of the following symptoms are observed.
- Children can have difficulty in reading small letters on the blackboard
- Some children squeeze their eyes while trying to see distant objects like blackboard, television etc.
- Children hold books close to their face while reading
- They can experience eye strain while trying to read for long hours.
- Some children with hyperopia can present with squint.
- Children can develop swellings on the lids due to constant rubbing of the eyes to see things clearly.
- Eye pain and headache may occur.
What are the types of Refractive Errors?
The refractive errors can be classified as myopia (near sightedness), hyperopia (far sightedness) and astigmatism.
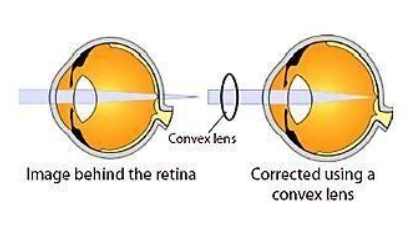
What is hyperopia?
In hyperopia or farsightedness, the light rays from an object form an image behind the retina. This happens commonly due to the size of the eyeball being smaller than normal.
Children with hyperopia;
- Find difficulty in reading, writing and looking at both near and distant objects.
- Face eye strain while trying to read for long hours
- may have squint (crossed eyes)
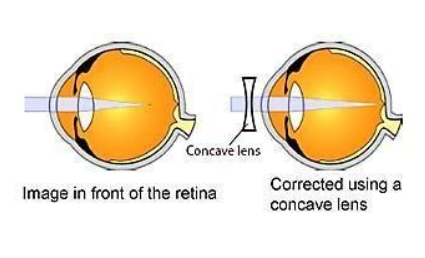
What is myopia?
In myopia or near sightedness, the light rays from an object form an image in front of the retina. This happens due to the eyeball being larger in size than normal.
Children with myopia;
- Have defective vision for distance and clear vision for near
- Squeeze their eyes while trying to see distant objects
- Hold books close to their face while reading
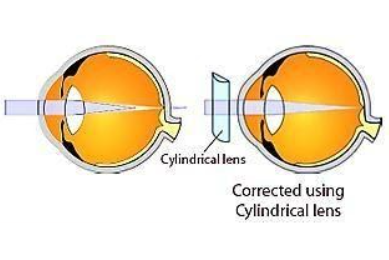
Astigmatism
This occurs due to changes in corneal curvature. The uneven focusing of the light on the retina distorts the image and makes it blurred. This condition is frequently seen in children with allergic eye conditions.
Children with refractive errors may also;
- Rub their eyes constantly or blink frequently, because of the eye strain which they experience all the time or have pain, watering or burning sensation in the eyes
- Have headache in the forehead region which gets intensified in the evening have recurrent swellings in the eye lids.

Presbyopia
Presbyopia occurs due to loss of ability of the lens in your eye to change its shape. As a result light coming from nearby objects does not focus on to the retina causing difficulty in doing near work (reading, writing, etc…) for the patient. This condition is a natural part of aging process and is commonly seen after the age of 40.
Patients with Presbyopia commonly present with eye strain and fatigue especially by the end of the day.
What are the treatment options for refractive errors?
Refractive errors can be treated by way of spectacles, contact lenses and / or refractive surgery.
Spectacles / Glasses:
- Correction using spectacles is the best option available. Though children may initially refuse to accept glasses, they will become fond of them once they realize that they can see better with the spectacles.
- The power of the glasses may change depending on the growth of the eye ball. An eye check-up (and change of glasses if necessary), has to be done once in 6 months for children under 5 years of age and once a year thereafter. Making a child wear glasses regularly is the duty and responsibility of the parents.
Contact Lenses
- Children older than 15 years can use contact lenses if they don’t want to use spectacles. Those over 18 to 20 years of age with stable power also have the option of LASIK, a laser refractive surgery apart from contact lenses.
Pros and Cons of Glasses / Contact Lenses
Glasses:
Pros:
- Relatively low maintenance
- Cheaper in the long term
- While wearing glasses, you are less likely to touch or rub your eyes. This reduces the risk of infection
- Everybody can wear glasses
- Glasses protect your eyes from dust, smoke, etc.
Cons:
- Glasses are available in many shapes, sizes, and colours and are often used to make a style statement!
- Side vision may be obstructed or blurred
- Glasses fog up in cold weather. Vision can also be blocked by rain
Contact Lenses:
Pros:
- The lens will take the shape of your eye. This gives a wider field of vision with fewer obstructions.
- Easier to exercise and play sports
- Lenses are not affected by weather. They should not fog up in the cold.
- They are less noticeable than glasses
Cons:
- Require proper lens care and cleaning. Contact lenses are in direct contact with your eye. Without proper care, you are at serious risk for infection
- They increase the risk of dry eye
- If you accidentally fall asleep with your contact lenses, your eyes will be very irritated when you wake up.
- In some specific eye conditions, it may be unsafe to use contact lenses
Refractive Surgery - LASIK
Refractive surgery as a treatment option for refractive errors can be offered to patients with stable eye power (those above the age of 18-20 years). The various refractive surgeries include LASIK (Laser Insitu Keratomileusis), phakic IOLs (intraocular lenses) and refractive lens exchange.
LASIK is the most commonly performed refractive surgery. It is a high-tech outpatient surgical technique for the treatment of myopia, astigmatism and hypermetropia. Utilising the accuracy and precision of the computer controlled excimer laser, LASIK changes the shape of the cornea and corrects refractive errors.
To know more about LASIK and other refractive surgeries click here.
Failure to correct the refractive errors and the eventual low vision may hamper the academic activities of the child. . Failure to wear glasses in childhood when needed will retard the development of vision in that eye, leading to amblyopia / lazy eye.
It can also lead to squinting of the eyes. So an ophthalmic consultation is essential in children, especially with symptoms of refractive errors.
Finally, there is no relationship between nutritional deficiency and the occurrence of refractive error. So loading these children with Vitamin A will not help them. Sometime this may lead on to other complications
What is Amblyopia?
Amblyopia is reduced vision in an anatomically normal eye. The term “lazy eye” is used to describe it.

What causes Amblyopia?
Amblyopia develops due to following factors:
- Squint / Strabismus (eyes not positioned straight) – In squint, amblyopia develops because when the eyes are misaligned, two different images are sent to the brain. In a young child, the brain learns to ignore the image of the deviated eye and see only the image of the better eye.
- When there is a difference in power between the two eyes (one eye focuses differently from the other), the blurred image formed by the eye with greater power is avoided by the brain, leading to development of amblyopia.
- When the child has cataract (clouding of the lens) / severe ptosis (droopy eyelids), adequate light and visual stimulus does not reach the retina resulting in amblyopia.
- A moderate or high degree of refractive power present in both eyes, when not corrected early and adequately, also results in amblyopia.
Children under 9 years of age whose vision is still developing are at the highest risk for developing amblyopia. Generally, the younger the child, the greater the risk.
How is Amblyopia diagnosed / detected?
Often, parents and children are unaware of the condition. Most parents do not take their children for an eye examination early in life and many children go undetected until they have their eyes examined at a later age. The most important diagnostic tool for amblyopia detection is visual acuity testing.
A complete eye examination is warranted which includes vision testing followed by refraction (with and without using eye drops) to rule out presence of any refractive error (hypermetropia, myopia or astigmatism). The alignment of the eyes is assessed to rule out squint. This is usually followed by a general structural examination of the eyes using slit lamp (microscope) and ophthalmoscope.
How is Amblyopia treated?
The most effective way of treating amblyopia is to make the child use the amblyopic eye, so as to ensure equal and normal vision. This can be achieved by:
- Glasses / Contact lenses – glasses play a major role in treating amblyopia to correct the refractive error. In some cases were one eye has higher refractive error than the other eye, the use of contact lenses can be of greater value than glasses.
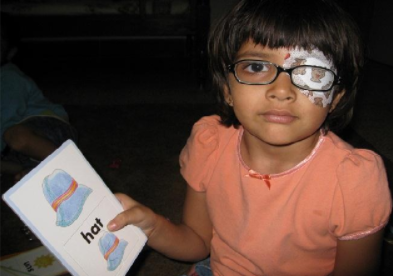
- Eye Patching – Eye patches are used to occlude the eye with better vision and stimulate the lazy eye to see more. The eye with better vision is patched / occluded with the help of biocompatible eye patch with the proper refractive correction in front of the amblyopic eye. In some children both are eyes are required to be patched alternately. Duration of patching of eyes varies depending on severity of the condition (treatment may extend from months to years). The ophthalmologist will decide for how long the occlusion should be continued. Loss of vision from amblyopia is preventable if treatment is begun early.
- Eye Exercises – There are some computer based apps were in the child is required to play a video games and / or solve puzzles in a supervised manner wearing 3D glasses so as to stimulate the amblyopic eye to see better.
- Eye Drops – Children who are uncooperative for patching of eyes can be administered with certain mydriatic eye drops (Atropine) for the eye with better vision so as to blur its vision temporarily. This way the lazy eye / amblyopic eye is stimulated / forced to see.
- Surgery – Certain children with cataract / squint / ptosis (drooping of eyelids) / corneal opacity require surgical intervention before institution of any of the above mentioned treatments for amblyopia.
How should one care for a child wearing a patch?
- Patching is not a pleasant thing for a child, so initially the child will be reluctant to undergo it. It is our duty to make the child understand the necessity of the procedure so that he/she will cooperate.
- In a young child patching is done for shorter periods initially; the duration is increased gradually to obtain better compliance.
- Acceptance is good as soon as vision improves in the amblyopic eye.
How should patching be done?
- Patch should be stuck directly on the face over the eye.
- If the child wears glasses, the patch should be placed on the face, not on the glasses.
- Glasses can also be used as an occluder only in older children.
- Many children try to take the patch off. This problem usually disappears as the child grows accustomed to wearing the patch.
- Older children can be encouraged to read and young children can be involved in playing interesting games during patching.
- Precautions must be taken to prevent the child from peaking around the edge of the patch.
- Patching schedules should be followed strictly.
- Patching should not be stopped abruptly. The programme should be tapered only by ophthalmologists.
Failure to correct refractive error leads to decreased vision and also hampers the academic activities of the child.
Children found with symptoms of refractive errors should be brought to an ophthalmologist for necessary correction.
Parents should encourage their children to wear glasses. Wearing glasses is not a stigma.
Loading children with vitamin A may neither help in preventing nor correcting refractive errors.
Spectacles themselves do not increase or decrease the power of the eye.
Amblyopia can often be reversed if it is detected and treated early.